Familial Hypercholesterolemia
What is Familial Hypercholesterolemia?
Familial Hypercholesterolemia (abbreviated as FH) is an inherited disorder in which people have high levels of a type of cholesterol called low-density lipoprotein (LDL or “bad cholesterol”) in their blood. This can lead to heart attacks and strokes at a young age, if left untreated.
Familial means that FH runs in families. It is often possible to trace FH over several generations.
Hypercholesterolemia means high blood cholesterol.
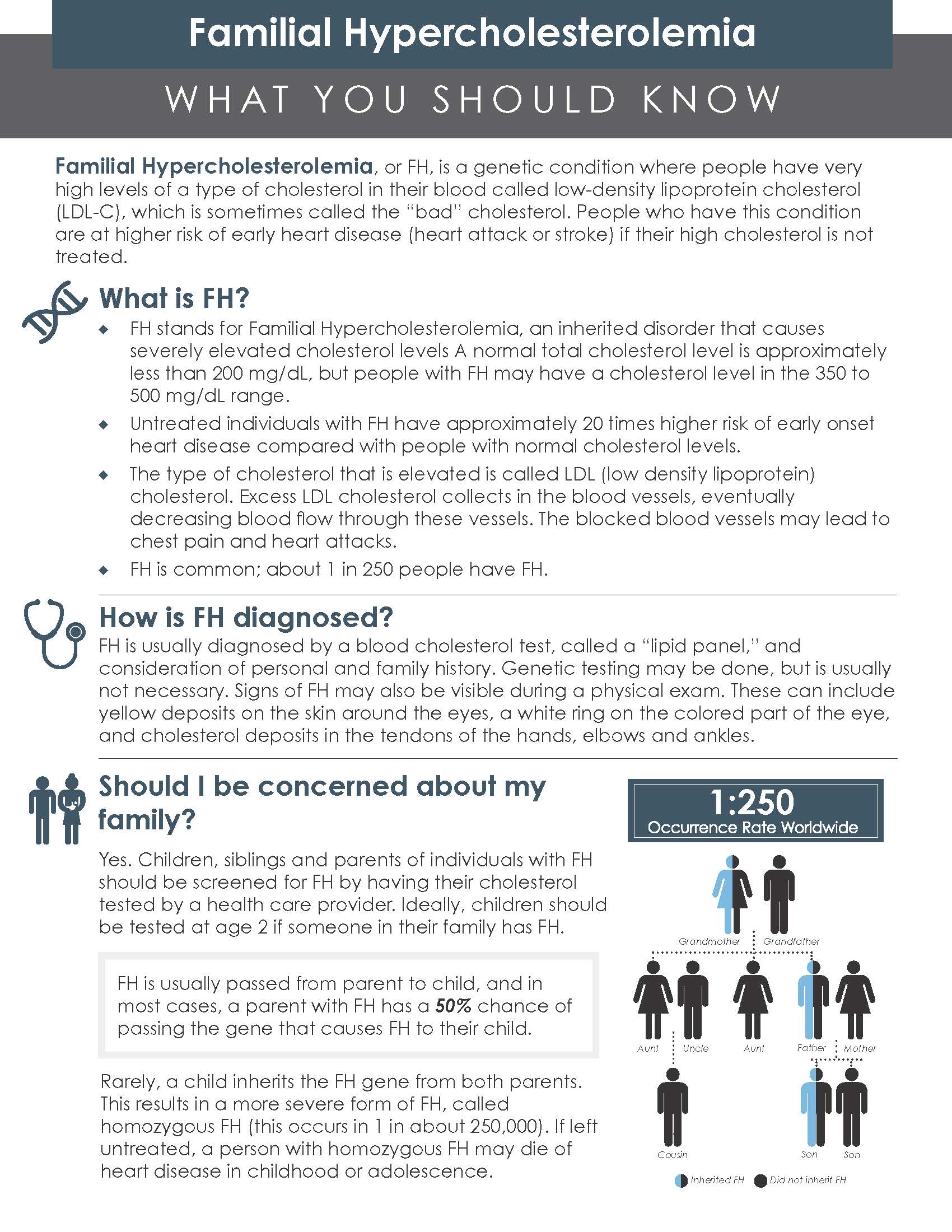
- FH is usually passed on from parent to child.
- FH patients have changes in their genes called mutations.
- These changes limit the body’s ability to remove cholesterol from the blood. This cholesterol then deposits in the walls of arteries forming fatty deposits called plaques which can block the arteries and lead to heart attacks and strokes.
- FH can either be heterozygous or homozygous.
- Heterozygous FH is caused by inheriting a changed gene from one parent only, meaning there will be one FH gene and one normal gene. It is common and affects about 1 in 300 people. Homozygous FH patients have two changed genes, usually one from each parent. It is much more severe and occurs in about 1 in 250,00 people. ( see pediatric lipid disorders).
- Like most chronic conditions such as diabetes and high blood pressure, patients with FH look perfectly healthy, and may not even realize that they have this problem.
Diagnosis
FH can be diagnosed by a blood cholesterol test, called a “lipid panel”, along with detailed personal and family history of heart disease and stroke. Although genetic testing is not always necessary, it can confirm the presence of mutations associated with FH. People with FH do not have any symptoms, but a physical exam may show signs of high cholesterol levels. These include a white ring on the colored part of the eye called arcus corneae, cholesterol deposits in the skin around eyes and knees as well as in the tendons of ankles, hands and elbows called xanthomas.

Clinical Criteria
Although there are different ways of making the diagnosis of FH, the American Heart Association has proposed the following criteria for heterozygous FH that can be used to diagnose FH:
- An untreated LDL-C >190mg/dl and either a first degree relative with LDL-C >190 or with known premature coronary heart disease (55 years in men and <60 years in women)
- Genetic testing with a mutation associated with FH
Criteria for homozygous FH:
- Untreated LDL-C over 400mg/dl
- Skin or tendon xanthomas before the age of 10 years and untreated elevated LDL-c levels consistent with heterozygous FH in both parents
Testing close family members enables early detection of the disease.
Lifestyle Recommendations
Diet
Patients with FH should follow a heart healthy diet. This means eating more fruits, vegetables, whole grains and lean proteins (like tofu, fish, Greek yogurt, beans, lentils, egg whites) and limiting saturated and trans fats such as high fat meats (prime rib, pork steaks, bacon, sausage); full fat dairy products; solid fats such as butter and coconut oil; fried foods, and many processed snacks.
Exercise
Aim to get 150 minutes of moderate intensity physical activity such as walking or 75 minutes of vigorous physical activity such as running every week, spread out over the week.
Weight Management
Maintain a healthy weight through diet and exercise.
Focus On
- Limiting Alcohol to moderate consumption which is up to one drink per day for women and two drinks for men. However, new guidelines suggest that lower amounts of alcohol are better.
- Avoiding smoking or use of any other tobacco products.
- Managing stress such as with the help of meditation, yoga and breathing exercises
- Taking your medications and getting your cholesterol levels checked regularly. These are also important parts of lifestyle.
- Getting enough sleep.
Treatment
The goal of treatment of FH is to lower the LDL cholesterol level. This can decrease the buildup of plaque in arteries. Lowering LDL cholesterol can prevent heart attacks and strokes. We want LDL cholesterol to be less than 100 mg/dL in people without heart disease and less than 70mg/dl in people who have had a heart attack or stroke or known vascular disease such as blockages to the legs or evidence of plaque on scans such as coronary artery calcium scans.
Medications
- Statins are the main treatment for FH and are the first to be used/prescribed. They work by blocking an enzyme in the liver that is involved in making cholesterol. Examples include atorvastatin (Lipitor) and rosuvastatin (Crestor)). Sometimes, patients complain of muscle aches, but most people can take statins at some dose. They are pills taken once a day. They can be taken anytime of the day, with or without food.
- Ezetimibe is an add-on therapy to statins but can be used by itself. This medication works by reducing cholesterol absorption from the diet. It is a once-a-day pill, taken with or without food. It has few side effects, such as stomach pain, gassiness, and diarrhea, which are rare.
- PCSK9 Inhibitors: There are two kinds. One type is an injectable medication taken once every two to four weeks. The two available ones are evolocumab (Repatha) and alirocumab (Praluent). They work by blocking a protein that affects the way LDL receptors work in the liver. LDL receptors are proteins on cells that pick up LDL particles and bring them into the cell. PCSK9 attaches to the LDL receptor and keeps it from recycling so that it can keep working. Blocking PCKS9 causes LDL receptors to work better leading to increased removal of LDL and reducing levels in the blood. Another type PCSK9 inhibitor is inclisiran. This is an injectable medication that keeps the liver from making PCSK9. It is given once every 6 months after two doses three months apart.
- Bile Acid Sequestrants: These drugs work by binding bile acids (made in the liver and put in bile for use in digestion) in the intestine, leading to lower cholesterol levels. They are cholestyramine, colestipol and colesevelam.
- Lomitapide: used for adults with homozygous FH. It works by reducing production of particles in the liver called VLDL. When these particles are sent out of the liver, they can be made into LDL particles.
- Evinacumab is an antibody to a protein that affects the body’s removal of LDL. It is given as an intravenous infusion once per month. It is only approved for people with homozygous FH, aged 5 and above.
Treatment Option
LDL apheresis is a treatment that can be used to help patients who are unable to reach their target LDL-c even with medications and lifestyle changes. During this procedure, blood is removed from the body and sent through a machine that filters LDL. The cleaned blood with much lower LDL levels, is then returned to the body. This entire process takes about 2-3 hours.
Lipid Specialist
Referral to a Lipid Specialist is useful for people with FH. Many patients with heterozygous FH will need more than one cholesterol lowering medication. Patients with homozygous FH may need multiple medications and may need LDL apheresis. You can search for a local lipid specialist through our website: https://www.learnyourlipids.com/find-a-clinician/.
Clinical Trials
A Phase 2 Clinical Study in Children With HeFH Aged 6 to 17 Treated Once Daily With Bempedoic Acid Oral Dosing (CLEAR Path 1)
ClinicalTrials.gov ID NCT05694260
Sponsor Esperion Therapeutics, Inc.
Additional Resources

What is Familial Hypercholesterolemia?
An essential, printable guide to Familial Hypercholesterolemia covering definitions, criteria, sub-categories, treatment options, impacts and additional resources.
Created through NLA partnership with PCNA.
